




This is a basic science study being done at Christian Medical College Hospital, Vellore in coordination with Copenhagen University, Copenhagen, Denmark and Steno Diabetes Centre, Copenhagen, Denmark.
It involves determining the baseline characteristics and the prospective impact of exercise in young South Indian males on –
- Insulin Resistance assessed by hyperinsulinemic euglycemic clamp technique.
- Body Composition as assessed by DEXA scanning.
- Skeletal Muscle and Hepatic Triglyceride Content as assessed by ¹H Nuclear Magnetic Resonance Spectroscopy.
- Energy Expenditure as assessed by Indirect Calorimetry.
It is well established that South Asians, who comprise more than one-fifth of the worlds population are more likely to develop insulin resistance, type 2 diabetes, hyperlipidemia and coronary artery disease (the metabolic syndrome x) when compared with the Western population.
What is the initial trigger for the development of metabolic syndrome in South Asians?
Several studies have shown epidemiological associations between poor foetal growth and subsequent development of Type 2 diabetes mellitus and the metabolic syndrome.
 Low birth weight and malnutrition in the intrauterine environment has been hypothesized to be an important factor in the development of metabolic syndrome.
Low birth weight and malnutrition in the intrauterine environment has been hypothesized to be an important factor in the development of metabolic syndrome.
The study has two cohorts of subjects aged 18-22 years, one cohort being previously normal birth weight and the other cohort having previously low birth weight subjects from a rural part of Tamil Nadu.
The aim of this study is to characterize metabolic differences between young Indian men born with low birth weight and born with normal birth weight with focus on Insulin secretion, Insulin resistance and body fat distribution. If an impaired secretion or action or a defect in energy expenditure is proven in Indians with low birth weight compared to normal birth weight Indians, then it may provide a better understanding of the biology of metabolic programming in utero. This is vital in preventing the epidemic of insulin resistance, obesity and type 2 diabetes mellitus in the vulnerable Indian phenotype and may warrant preventive health care strategies targeting such population at an earlier age.
Hyperinsulinemic Euglycemic Clamp technique
This is considered as the gold standard for quantifying Insulin sensitivity. The duration of the procedure is 2 hours during which the patient receives an Insulin infusion so as to acutely raise the plasma Insulin and then maintain at 100 micro units/ml. Simultaneously a variable glucose infusion to maintain euglycemia is given. Blood Glucose estimation by glucometer is done every five minutes to assist making changes in glucose infusion rate. A steady state is reached during which the glucose infusion rate is equal to the rate at which glucose is disposed by Insulin (maximal insulin stimulated glucose uptake by tissues). It thus gives us a measure of tissue sensitivity to Insulin. High levels of glucose infusion needed during the steady state to maintain euglycemia mean tissue sensitivity to Insulin and low infusion rates signify resistance to the action of Insulin. The M value or the Insulin sensitivity is calculated as average of the glucose infusion rates (mg/min) during the last half hour of the clamp divided by the fat free mass (kg) as determined by DEXA scan.
Indirect Caloriemeter


Actiheart
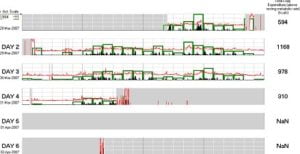 The Actiheart logger consists of a larger, round, main sensor and a lead to the positive electrode lead typically worn on the left side of the chest. Both sensor leads affix to electrodes attached on to the chest wall at specific locations and pick up the ECG signal. The details of the subject are entered in to the actiheart’s database. The subject is sent home with the device and the data from the actiheart is downloaded after 3 days.
The Actiheart logger consists of a larger, round, main sensor and a lead to the positive electrode lead typically worn on the left side of the chest. Both sensor leads affix to electrodes attached on to the chest wall at specific locations and pick up the ECG signal. The details of the subject are entered in to the actiheart’s database. The subject is sent home with the device and the data from the actiheart is downloaded after 3 days.
The actiheart correlates heart rate and activity level (activity counts) data which it senses, and converts it in to energy units (calories) through an inbuilt program. It is thus a very useful device which provides us with a solid base to determine energy expenditure in a simple way.
Bicycle Ergometry
 The test uses an exercise bicycle which provides a graded increase in resistance over specified time periods. There is a 5 minute reference phase during which the patient cycles with a load of 10 watts and warms up. The test proper starts with a load of 50 watts and increases by 30 watts with every passing minute. The test goes on until the patient tires. It gives us an index of the subject’s exercise capacity.
The test uses an exercise bicycle which provides a graded increase in resistance over specified time periods. There is a 5 minute reference phase during which the patient cycles with a load of 10 watts and warms up. The test proper starts with a load of 50 watts and increases by 30 watts with every passing minute. The test goes on until the patient tires. It gives us an index of the subject’s exercise capacity.
A heart rate sensor worn around the chest gives information about the subject’s ability to reach maximal heart rate over the period of exercise. It is coupled with a breath by breath ergo-spirometry to determine energy expenditure by indirect Calorimetry. Blood lactate levels are measured immediately after the test. Measuring lactate during moderate exercise is a useful tool in the diagnosis of mitochondrial disorders. Thus we are looking to determine any defect with energy expenditure in our subjects.
